

![]()
 As surgeons that wear many different hats during the week (Cosmetic Surgery, Reconstructive Surgery, Bariatric Surgery, and General Surgery), Dr. Swetnam and I are faced with constant challenges; and it is a significant challenge to keep everyone satisfied. As one of my favorite subjects, today I'll discuss post weight loss cosmetic surgery.
As surgeons that wear many different hats during the week (Cosmetic Surgery, Reconstructive Surgery, Bariatric Surgery, and General Surgery), Dr. Swetnam and I are faced with constant challenges; and it is a significant challenge to keep everyone satisfied. As one of my favorite subjects, today I'll discuss post weight loss cosmetic surgery.
Typically, bariatric surgery patients first and foremost have decided to take the plunge in changing their lives. I heard it best this week from a patient who told me, "Dr. Miller, I am sick and tired of being sick and tired." It's a lifetime of habits that they must break: the way they eat, the way they exercise, even just the way they think. The positive repercussions of weight loss are legion. It truly is an entire lifestyle change. It is amazing for me to see how one positive change by a bariatric patient effects those around them. I recently saw a patient that was 12 weeks out from a sleeve gastrectomy.

To both of our satisfaction, he had already lost 70 pounds. On top of that, his wife had also lost 30 pounds just by following the same diet that I'd ask him to impart postoperatively. The little cherry on top of all this icing post surgery was that their daughter had also decided to begin to make healthy food choices, resulting in weight loss as well. It's amazing how one positive decision begets another positive decision. Unfortunately, one of the few anticipated post weight loss "problems" (besides having to purchase a new "skinny" wardrobe), is what to do with all the extra skin that sometimes results from losing excess weight...? The thing is, not everyone ends up with excess skin. Really, it depends on multiple factors: the patient's age (no, I didn't just call you old); how many children a patient may have had; excess roller coaster weight loss and gain over the year; and the personal skin elasticity of a patient. The latter really making the majority of the difference. Quite honestly, it really comes down to how you picked your parents when it comes to skin elasticity. Genetics is key to just about everything under the sun, and skin elasticity certainly falls into that category. So why does this matter? Think of it this way: if you have a 10 pound sack of potatoes and take out 9 pounds of those potatoes, you've got a lot of sack left over, right? Sometimes this sack shrinks down, and other times it does not. Again, all as a result (or lack thereof) of the degree of skin elasticity someone may or may not have. I am often asked if exercise will help to tighten up the skin. Unfortunately, I can assure you that all the situps and jogging in the world will not help that excess skin to shrink. So, what is the answer then? What do I do now that I've lost this weight and my skin gets rashes between the folds? And sure, I've lost a significant amount of weight, but my clothes still don't fit right lugging this extra skin around! This is where the post weight loss recontouring comes into play.
Though not every post weight loss patient needs them, there are multiple body contouring options for those that do post weight loss: tummy tucks, liposuction, arm lifts, breast lifts, thigh lifts, and body lifts. Typically, one or a combination of these procedures have been successfully used after weight loss surgery to refine patients’ bodies, and help them enjoy everyday activities as they envisioned at the beginning of their journey. The most common procedure that Dr. swetnam and I do is the tummy tuck. Essentially, that entails not just removing the excess skin present, but also tightening up the actual abdominal muscles. We basically create an internal corset that results in a waist that many people had not seen for many, many years. Following the tummy tuck, I would say that breast lifts are our next most common procedure post weight loss. It's amazing to see how people's attitudes change as they continue along their weight loss journey. Specifically, people who had become shy wall flowers virtually become alive again. Their inner personality that had been stifled for so long is reawakened. No longer just satisfied to wear bulky sweaters and oversized tshirts to hide their insecurities, they sometimes pursue breast lifts. Breasts that were once being tucked into their front pockets are now perky and full on the top of their chest- right where they should be. Following breast lifts, arm lifts (sometimes termed brachioplasty in doctor-ese) would be the next most common procedure that Dr. swetnam and I perform. It is essentially just removing extra skin and remaining fat to create a nicely contoured arm again. Thigh lifts are much like arm lifts, except just a bit further south. I would say that thighs are the most challenging to operate on, as God didn't create us in anticipation of having incisions in our groins (location required to lift up those thighs again). I should mention here that the great thing about having two fellowship trained cosmetic surgeons together in a group means that more procedures can be done at the same time. Why does that make any difference? First and foremeost, the operative time is more than halved. This is not just better for the patient's health, but also is more cost friendly for the patient in the long run.

So when should a post weight loss patient consider having body contouring procedures done? Typically, I suggest that a patient be within 80% of their weight loss goal. Typically, this is at sometime between 12 and 18 months. As I said, body contouring is not something that is essential from a health perspective, but rather as the end result of a long journey. It's basically seeing the final end point result come to fruition. It has been said more than once that we are flattered to be a part of this whole process, both as the wearing the weight loss surgeon's hat, as well as that of the body recontouring surgeon's. We literally know our patients inside and out!
Come see us today for your complimentary Cosmetic consultation!! 918-786-7780 or 1-877-weight-0.


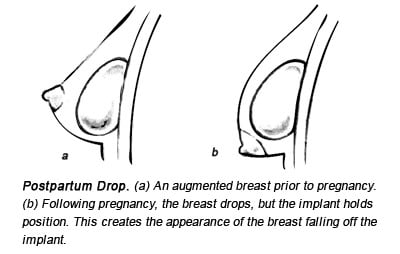


 In this picture, the nipple position is great, the skin is tight, and only an implant is necessary. After implant placement, the skin will stretch to accomidate the implant and the breast will take on a nice and natural shape. This is the perfect patient for implants alone. As discussed in earlier blogs, the incision placement options, size, and type of implants are variable according to taste. At your consult, all of this will be discussed and you can decide.
In this picture, the nipple position is great, the skin is tight, and only an implant is necessary. After implant placement, the skin will stretch to accomidate the implant and the breast will take on a nice and natural shape. This is the perfect patient for implants alone. As discussed in earlier blogs, the incision placement options, size, and type of implants are variable according to taste. At your consult, all of this will be discussed and you can decide. This picture depicts one of the "easy" decisions. Obvious drooping of the breast and nipple complex below the lower fold of the breast where it attaches to the chest. If we were to just place an implant in this situation, there would be a nice implant present with a sagging breast hanging off with the nipple still pointing at the floor. Several procedures are used to lift the breast. We usually use the Weiss pattern lift (anchor incision) for larger lifts and the vertical (lolly pop) lift. Both types of lift raise the nipple into a more normal position, remove excess skin below the breast and move remaining breast tissue into a higher position. In the picture above, we call this the "rocks in socks" breast. There is some breast tissue hanging around the nipple (rocks), and skin (socks). If lifted only, this will be a very small and flat breast. This is when an implant can really be beneficial to give the breast some volume. Others have a sagging nipple and breast but still have a good amount of volume. A lift alone, or with implants are both choices.
This picture depicts one of the "easy" decisions. Obvious drooping of the breast and nipple complex below the lower fold of the breast where it attaches to the chest. If we were to just place an implant in this situation, there would be a nice implant present with a sagging breast hanging off with the nipple still pointing at the floor. Several procedures are used to lift the breast. We usually use the Weiss pattern lift (anchor incision) for larger lifts and the vertical (lolly pop) lift. Both types of lift raise the nipple into a more normal position, remove excess skin below the breast and move remaining breast tissue into a higher position. In the picture above, we call this the "rocks in socks" breast. There is some breast tissue hanging around the nipple (rocks), and skin (socks). If lifted only, this will be a very small and flat breast. This is when an implant can really be beneficial to give the breast some volume. Others have a sagging nipple and breast but still have a good amount of volume. A lift alone, or with implants are both choices. This is a photo of a breast lift alone. The shape is nice and nipple position is good, however, the upper pole remains flat. This can only be fixed, long term, with an implant. Implants, however, can be placed after a lift so you can decide later if you want them or not.
This is a photo of a breast lift alone. The shape is nice and nipple position is good, however, the upper pole remains flat. This can only be fixed, long term, with an implant. Implants, however, can be placed after a lift so you can decide later if you want them or not. As you can see, a lift with an augmentation can be done simultaneously with good results. This gives good fullness to the upper pole of the breast with the added benefit of only one procedure.
As you can see, a lift with an augmentation can be done simultaneously with good results. This gives good fullness to the upper pole of the breast with the added benefit of only one procedure. Breast pseudoptosis with implants. Looks pretty good, but upper pole is somewhat flat. If this is acceptable, it is a great choice.
Breast pseudoptosis with implants. Looks pretty good, but upper pole is somewhat flat. If this is acceptable, it is a great choice.


 Capsular contracture on right with implant thightening and displacement. It would feel very hard if you could feel it.
Capsular contracture on right with implant thightening and displacement. It would feel very hard if you could feel it. implant "rippling"
implant "rippling"

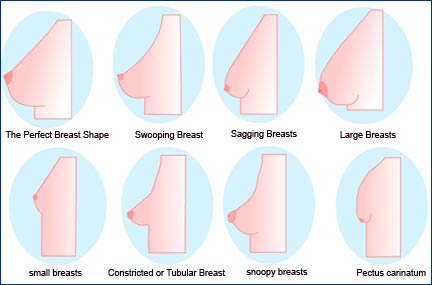
 (the "perfect" breast shape is a misnomer of course)
(the "perfect" breast shape is a misnomer of course)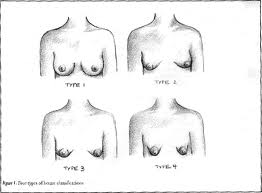 This picture is a depiction of tubular breasts of different severities. It is the mound of the breast that is constricted and does not spread out, therefore, the tubular shape of the breast.
This picture is a depiction of tubular breasts of different severities. It is the mound of the breast that is constricted and does not spread out, therefore, the tubular shape of the breast.  Herniated "puffy" nipple.
Herniated "puffy" nipple.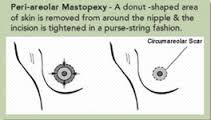 This incision allows us to reduce the nipple size and when closed it flattens the nipple and areola into a more normal appearance. The constricted breast is broken up below so that it is no longer in a tube shape and lays flatter.
This incision allows us to reduce the nipple size and when closed it flattens the nipple and areola into a more normal appearance. The constricted breast is broken up below so that it is no longer in a tube shape and lays flatter.  Good representation of tubular breast deformity repair.
Good representation of tubular breast deformity repair.
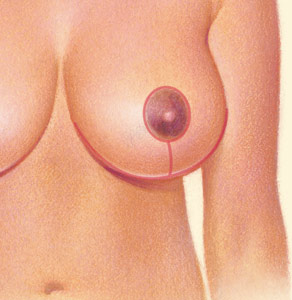 The nipple is not "removed", it is rotated into its new spot conserving the nervous innervation and blood supply. These incisions have a tendency to heal very well and after 6-12 months they turn into little white lines. Implants, saline or silicone, are placed through the same incisions and usually under the muscle so they stay in place over time.
The nipple is not "removed", it is rotated into its new spot conserving the nervous innervation and blood supply. These incisions have a tendency to heal very well and after 6-12 months they turn into little white lines. Implants, saline or silicone, are placed through the same incisions and usually under the muscle so they stay in place over time. Some can get away with a mini tummy tuck which removes a small amount of sagging skin (below the belly button) only.
Some can get away with a mini tummy tuck which removes a small amount of sagging skin (below the belly button) only.
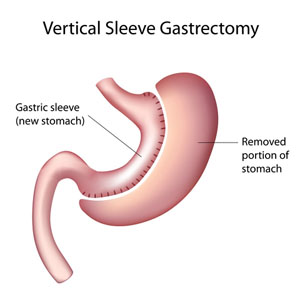 The gastric sleeve decreases the amount of food that can be consumed when eating a meal. It also decreases the amount of the hormones produced by the stomach that causes hunger and the desire to eat. This is a proven procedure that is done through the laparoscope with an over night stay in most cases. The weight loss is dramatic with no adjustments.
The gastric sleeve decreases the amount of food that can be consumed when eating a meal. It also decreases the amount of the hormones produced by the stomach that causes hunger and the desire to eat. This is a proven procedure that is done through the laparoscope with an over night stay in most cases. The weight loss is dramatic with no adjustments. 

 We can lift the breast in this instance but it will not make the upper part of the chest full. Once the nipple has been repositioned into a more appropriate spot, we have all the skin left below it. This skin must be removed and the skin envelope tightened. We now have a breast that is much perkier with a nipple position that is elevated.
We can lift the breast in this instance but it will not make the upper part of the chest full. Once the nipple has been repositioned into a more appropriate spot, we have all the skin left below it. This skin must be removed and the skin envelope tightened. We now have a breast that is much perkier with a nipple position that is elevated.  As you can see, there is a great improvement in shape and nipple position. However, from this 45 degree view, the upper aspect of the breast is very sloped. Many women don't mind this and that is fine but if upper breast fullness is desired an augmentation is required with an implant. That's where the problem comes in. The second problem is this; now that we have a tighter breast skin envelope we are now going to place an implant that will stretch what we have now tightened. This can easily be done and since we have lifted the nipple we put the implant below the muscle. What this does is fill in the upper pole of the breast and helps you regain that youthful breast that was lost.
As you can see, there is a great improvement in shape and nipple position. However, from this 45 degree view, the upper aspect of the breast is very sloped. Many women don't mind this and that is fine but if upper breast fullness is desired an augmentation is required with an implant. That's where the problem comes in. The second problem is this; now that we have a tighter breast skin envelope we are now going to place an implant that will stretch what we have now tightened. This can easily be done and since we have lifted the nipple we put the implant below the muscle. What this does is fill in the upper pole of the breast and helps you regain that youthful breast that was lost.
